
This post is part of a series of guest posts on GPS by the graduate students in my Psychopathology course during Spring 2014. As part of their work for the course, each student had to demonstrate mastery of the skill of “Educating the Public about Mental Health.” To that end, each student has to prepare two 1,000ish word posts on a particular class of mental disorders, with one of those focusing on evidence-based treatments for those disorders and the other focused on a particular myth or misunderstanding about mental illness.
______________________________________________
Female Sexual Dysfunction: Myth or Mental Illness? by Lauren Reed
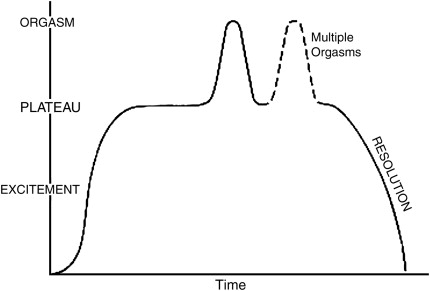 Sexual dysfunctions have been considered mental illnesses since the release of the DSM-III in 1980. While the terms and criteria changed slightly over the next few decades, the model used to determine sexual dysfunctions remained consistent. The sexual response cycle described by Masters and Johnson contained four phases of the human sexual response cycle: excitement, plateau, orgasm, and resolution. This traditional, linear model was used to describe the sexual functions for both males and females. As it turns out, these four phases are not very representative of actual sexual functioning, especially female sexual functioning. Bringing the validity of this model into question, the new DSM-5 completely abandoned this model and moved towards a gender-specific classification of sexual dysfunctions. These disorders are now commonly referred to as Male Sexual Dysfunctions (MSD) and Female Sexual Dysfunctions (FSD).
Sexual dysfunctions have been considered mental illnesses since the release of the DSM-III in 1980. While the terms and criteria changed slightly over the next few decades, the model used to determine sexual dysfunctions remained consistent. The sexual response cycle described by Masters and Johnson contained four phases of the human sexual response cycle: excitement, plateau, orgasm, and resolution. This traditional, linear model was used to describe the sexual functions for both males and females. As it turns out, these four phases are not very representative of actual sexual functioning, especially female sexual functioning. Bringing the validity of this model into question, the new DSM-5 completely abandoned this model and moved towards a gender-specific classification of sexual dysfunctions. These disorders are now commonly referred to as Male Sexual Dysfunctions (MSD) and Female Sexual Dysfunctions (FSD).
Upon reading the history of Sexual Dysfunctions, it seems like FSD has always been present, it’s just been overshadowed by the progress and advancements made in MSD. At least, that’s exactly what the pharmaceutical companies want you to believe. So where did this all begin? Medicalization of human sexuality has been occurring over the past four decades without much question. As a society, we often think of a dysfunction as something abnormal, needing to be fixed. Pharmaceutical companies capitalize on this societal naiveté, producing “miracle drugs” to cure diseases and disorders that don’t even exist yet. Shortly after Pfizer released their magical blue pill for men, better known as Viagra, the hunt began for the female version of this “miracle drug”. It was unclear what this female version of Viagra was going to treat, but the race was on to be the first to discover the next multi-billion drug to cure this disease that didn’t exist yet.
Of course, in order to promote a drug that is going to cure women of this disease, awareness has to be brought to the population that suffers from this illness. Celebrity Oprah Winfrey held a segment in which FSD was discussed and described as a “secret epidemic”. This led many women to begin to question their sexuality and what they considered “normal”. Dr. Laura Berman emerged as an American sex educator and relationship therapist promoting the need to find effective medications to treat FSD. It appeared she had women’s best interest at heart and wanted to provide women the same sexual opportunities as men. What wasn’t so apparent was Dr. Berman’s affiliation with Pfizer and the clinical trials that were being conducted in the search for the female “miracle drug”. She forgot to mention that part of her income when promoting the need to find treatments to help women with FSD.
So what happened after this awareness was brought to the attention of women? Well, a study was conducted in which the prevalence rate of FSD in women was determined to be 43%. This alarmingly high rate can be taken in one of two ways. The first way to look at this high prevalence rate is through the eyes of a pharmaceutical company. Over 4 in 10 women suffer from an FSD. Therefore, research and funding needs to be geared toward solving this problem. It would be neglectful to ignore this “secret epidemic” that has finally surfaced. The second way to look at this high prevalence rate is through the eyes of a skeptic. If nearly half of the population of women have FSD, then is it really a dysfunction? Might this class of disorders be a result of medicalizing something that’s normal?
It seems society is in need of a bit of sexual education. As it turns out, women’s sexual experiences vary greatly. Sexual experiences don’t just vary between women, but also within one woman’s own sexual experiences. The DSM-5 has coined a specific FSD known as Female Orgasmic Disorder. The operational definition of this disorder is marked delay in, marked infrequency of, or marked absence of orgasm or markedly reduced intensity of orgasmic sensations. I hate to be the bearer of bad news, but not every sexual activity leads to orgasm. In fact, only about 30% of women climax with almost every sexual activity.
Another worry often associated with this disorder is lack of orgasm through vaginal penetration only. Because the female orgasm has been medicalized, women now think they have a dysfunction if they don’t orgasm in every sexual activity. Interesting enough, only about 20% of women experience orgasm with vaginal penetration only and most require clitoral stimulation to climax. The DSM-5 has also coined a FSD known as Female Sexual Interest/Arousal Disorder. Its operational definition is far too long to type here, so I will give you the brief version: absent/reduced sexual interest/arousal. It’s hard to grasp, I know, but sometimes women are just not interested in sex. It seems like we have taken these ordinary aspects of sexual functioning, such as decreased libido and arousal, and made them into something a pill might fix. Unfortunately, even the most “magical” pill can’t fix a disease that doesn’t actually exist.